
Stomatology ›› 2024, Vol. 44 ›› Issue (7): 515-521.doi: 10.13591/j.cnki.kqyx.2024.07.006
• Basic and Clinical Research • Previous Articles Next Articles
LI Gen1,2,GUO Songsong1,3,CAI Guanhui1,2,SUN Lian1,2,SUN Wen1,2,WANG Hua1,2,4( )
)
Received:2024-01-11
Online:2024-07-28
Published:2024-07-15
CLC Number:
LI Gen, GUO Songsong, CAI Guanhui, SUN Lian, SUN Wen, WANG Hua. Correlation between upper airway morphological changes and jaw movement after bimaxillary orthognathic surgery in patients with skeletal Class Ⅲ malocclusion[J]. Stomatology, 2024, 44(7): 515-521.
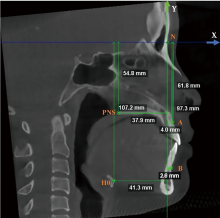
Fig.1
Landmark measurements"
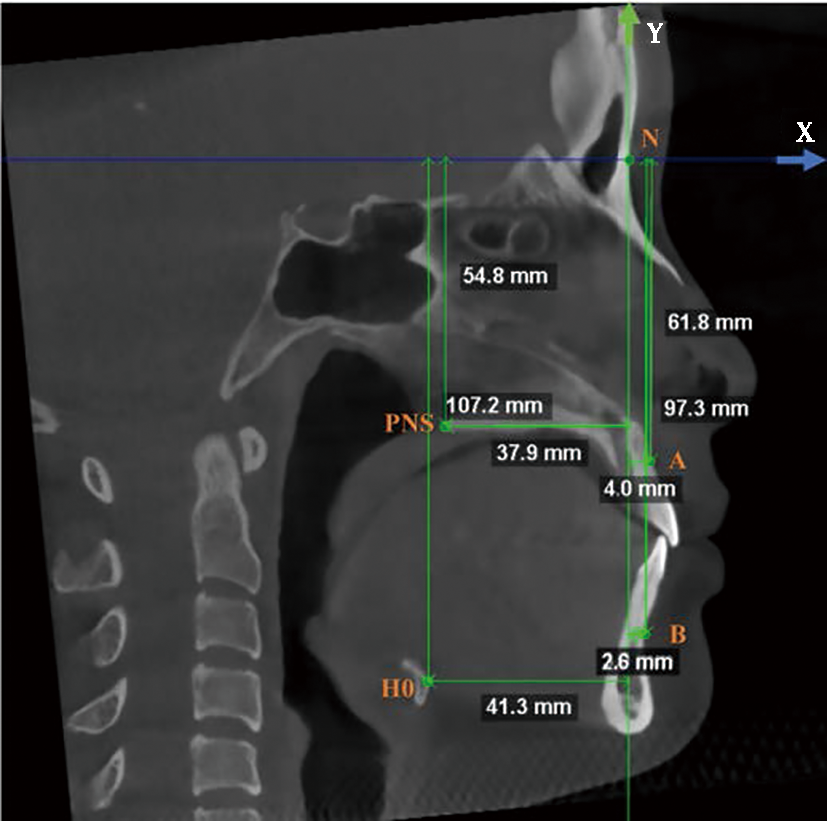
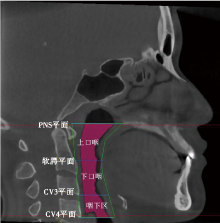
Fig.2
Upper airway boundaries"
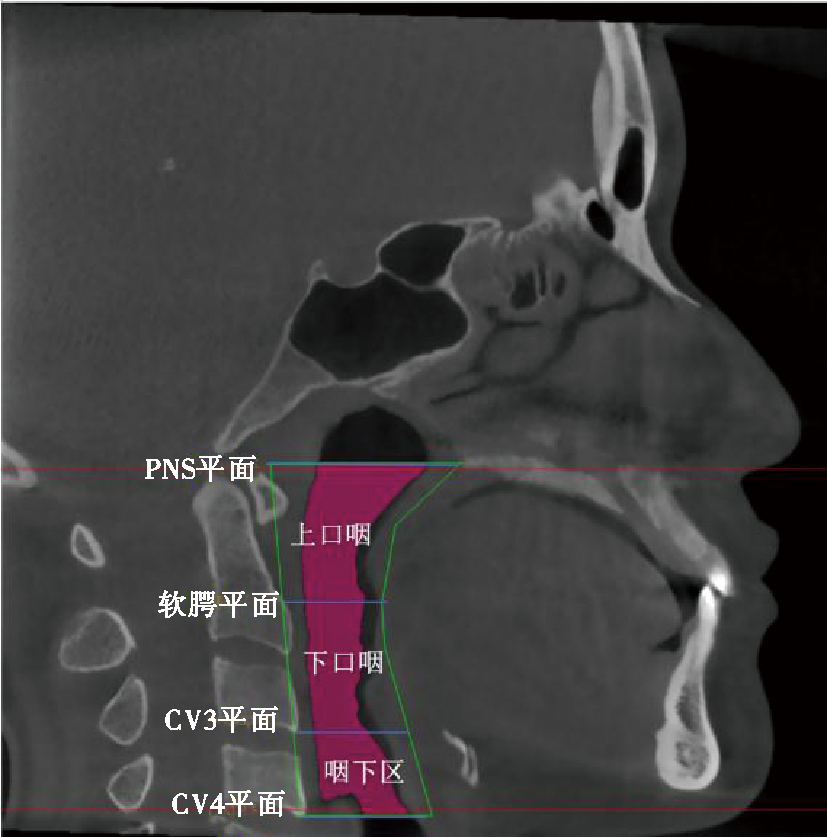
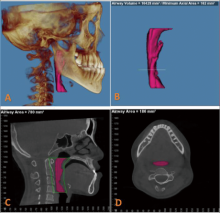
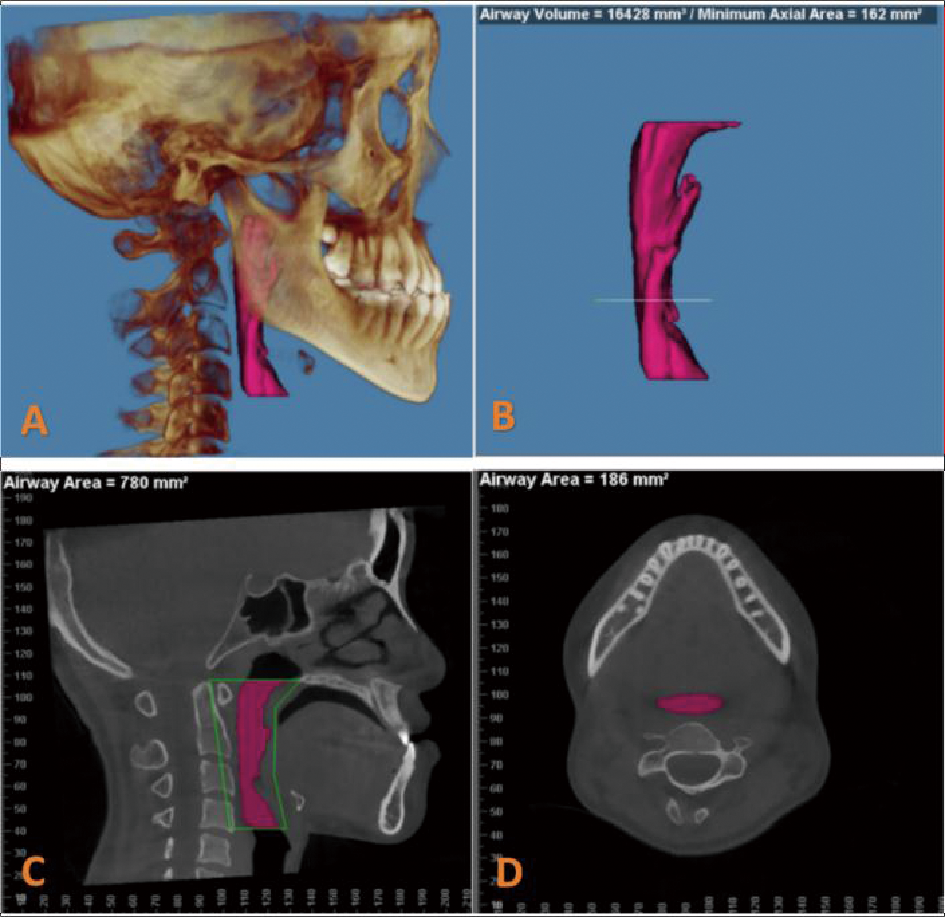
Fig.3
Airway measurement"
Tab.1
Changes in landmarks and cephalometric measurements before and after surgery"
| 测量项目 | 术前 | 术后 | 术后-术前 | P | ||||
|---|---|---|---|---|---|---|---|---|
| 平均值 | 标准差 | 平均值 | 标准差 | 平均值 | 标准差 | |||
| ANB/(°) | -4.03 | 2.64 | 0.77 | 1.96 | 4.80 | 2.12 | 0.000* | |
| wits值/mm | -12.13 | 3.65 | -3.98 | 2.97 | 8.16 | 2.82 | 0.000* | |
| A-Y轴/mm | 1.59 | 3.23 | 3.16 | 3.70 | 1.57 | 1.65 | 0.000* | |
| A-X轴/mm | -61.64 | 4.27 | -62.38 | 5.05 | -0.74 | 2.23 | 0.033* | |
| B-Y轴/mm | 8.88 | 5.68 | 3.39 | 5.29 | -5.49 | 3.24 | 0.000* | |
| B-X轴/mm | -101.14 | 8.02 | -99.98 | 6.99 | 1.17 | 3.02 | 0.014* | |
| PNS-Y轴/mm | -42.72 | 4.05 | -39.93 | 3.99 | 2.79 | 1.67 | 0.000* | |
| PNS-X轴/mm | -53.41 | 4.06 | -53.42 | 4.41 | -0.01 | 1.52 | 0.953 | |
| H0-Y轴/mm | -37.28 | 7.63 | -38.6 | 7.60 | -1.33 | 3.68 | 0.021* | |
| H0-X轴/mm | -113.35 | 8.51 | -115.73 | 9.57 | 2.38 | 4.69 | 0.002* | |
Tab.2
Differences in upper airway areas before and after surgery"
| 测量项目 | 术前 | 术后 | 术后-术前 | 变化率 | P | |||
|---|---|---|---|---|---|---|---|---|
| 平均值 | 标准差 | 平均值 | 标准差 | 平均值 | 标准差 | |||
| 气道体积/mm3 | ||||||||
| 总气道 | 2 1381.1 | 8 275.5 | 17 442.3 | 6 002.7 | -3 938.9 | 4 732.6 | -16.39% | 0.000* |
| 口咽区 | 15 745.0 | 6 576.9 | 12 525.2 | 4 745.4 | -3 219.8 | 3 845.9 | -17.88% | 0.000* |
| 上口咽区 | 8 307.7 | 4 039.5 | 6 585.0 | 2 902.3 | -1 722.8 | 2 475.0 | -17.24% | 0.000* |
| 下口咽区 | 7 539.2 | 3 274.5 | 5 837.0 | 2 509.8 | -1 702.2 | 2 240.4 | -19.15% | 0.000* |
| 咽下区 | 5 629.3 | 2 168.8 | 4 914.7 | 1 891.1 | -714.6 | 1 274.2 | -10.61% | 0.001* |
| 正中矢状面纵截面积/mm2 | ||||||||
| 总气道 | 943.6 | 208.2 | 842.7 | 180.4 | -100.9 | 130.8 | -9.87% | 0.000* |
| 口咽区 | 705.4 | 160.8 | 627.9 | 137.7 | -77.5 | 95.0 | -10.13% | 0.000* |
| 上口咽区 | 385.3 | 93.6 | 345.1 | 68.5 | -40.3 | 64.1 | -8.78% | 0.000* |
| 下口咽区 | 326.6 | 100.2 | 286.1 | 93.1 | -40.5 | 64.9 | -10.89% | 0.000* |
| 咽下区 | 236.5 | 71.3 | 218.4 | 61.5 | -18.0 | 53.9 | -3.53% | 0.032* |
| 最小横截面积/mm2 | ||||||||
| 总气道 | 171.6 | 79.1 | 121.5 | 59.1 | -50.1 | 57.5 | -23.32% | 0.000* |
| 口咽区 | 181.1 | 89.6 | 126.5 | 63.1 | -54.6 | 63.4 | -26.95% | 0.000* |
| 上口咽区 | 191.9 | 102.8 | 146.0 | 81.3 | -45.9 | 58.4 | -20.99% | 0.000* |
| 下口咽区 | 221.1 | 94.8 | 156.9 | 67.8 | -64.3 | 78.0 | -25.07% | 0.000* |
| 咽下区 | 229.3 | 113.6 | 202.3 | 95.7 | -27.1 | 92.9 | -0.65% | 0.060 |
Tab.3
Analysis of correlation between airway and jaw movement change"
| 测量项目 | 统计值 | A点矢状 向变化量 | A点垂直 向变化量 | B点矢状 向变化量 | B点垂直 向变化量 | PNS点矢状 向变化量 | PNS点垂直 向变化量 | H0点矢状 向变化量 | H0点垂直 向变化量 |
|---|---|---|---|---|---|---|---|---|---|
| 总气道体积 | rs | 0.099 | -0.061 | 0.461 | 0.163 | -0.067 | 0.120 | -0.187 | -0.041 |
| P | 0.524 | 0.693 | 0.002* | 0.290 | 0.667 | 0.437 | 0.225 | 0.792 | |
| 口咽体积 | rs | 0.111 | -0.043 | 0.431 | 0.231 | -0.066 | 0.128 | -0.221 | -0.050 |
| P | 0.474 | 0.783 | 0.004* | 0.132 | 0.670 | 0.407 | 0.150 | 0.747 | |
| 上口咽体积 | rs | 0.229 | 0.005 | 0.303 | 0.171 | 0.072 | 0.246 | -0.135 | -0.098 |
| P | 0.135 | 0.973 | 0.046* | 0.268 | 0.641 | 0.107 | 0.382 | 0.525 | |
| 下口咽体积 | rs | -0.027 | -0.203 | 0.356 | 0.103 | -0.108 | 0.058 | -0.221 | 0.048 |
| P | 0.861 | 0.187 | 0.018* | 0.505 | 0.487 | 0.709 | 0.149 | 0.758 | |
| 咽下体积 | rs | -0.180 | -0.004 | 0.283 | 0.066 | -0.240 | 0.107 | -0.066 | -0.197 |
| P | 0.241 | 0.979 | 0.063 | 0.668 | 0.116 | 0.488 | 0.669 | 0.200 | |
| 总气道纵截面积 | rs | 0.148 | -0.083 | 0.379 | 0.105 | 0.047 | 0.153 | -0.054 | -0.087 |
| P | 0.336 | 0.593 | 0.011* | 0.499 | 0.763 | 0.321 | 0.727 | 0.576 | |
| 口咽纵截面积 | rs | 0.241 | -0.071 | 0.392 | 0.159 | 0.062 | 0.158 | -0.131 | 0.03 |
| P | 0.115 | 0.646 | 0.009* | 0.302 | 0.690 | 0.306 | 0.396 | 0.848 | |
| 上口咽纵截面积 | rs | 0.249 | 0.051 | 0.201 | 0.095 | 0.213 | 0.305 | -0.144 | -0.085 |
| P | 0.103 | 0.744 | 0.191 | 0.540 | 0.165 | 0.044* | 0.351 | 0.583 | |
| 下口咽纵截面积 | rs | 0.022 | -0.102 | 0.313 | 0.136 | -0.145 | 0.028 | -0.231 | -0.013 |
| P | 0.887 | 0.509 | 0.039 | 0.380 | 0.348 | 0.856 | 0.131 | 0.932 | |
| 咽下纵截面积 | rs | -0.049 | -0.216 | 0.068 | -0.142 | -0.102 | 0.057 | -0.023 | -0.086 |
| P | 0.751 | 0.158 | 0.661 | 0.356 | 0.512 | 0.713 | 0.882 | 0.579 | |
| 总气道横截面积 | rs | 0.193 | 0.040 | 0.413 | 0.093 | 0.165 | 0.132 | -0.082 | 0.080 |
| P | 0.209 | 0.797 | 0.005* | 0.547 | 0.284 | 0.393 | 0.598 | 0.607 | |
| 口咽横截面积 | rs | 0.091 | 0.066 | 0.399 | 0.200 | 0.079 | 0.043 | -0.190 | 0.061 |
| P | 0.558 | 0.672 | 0.007* | 0.194 | 0.610 | 0.781 | 0.216 | 0.696 | |
| 上口咽横截面积 | rs | 0.199 | 0.000 | 0.434 | 0.219 | 0.112 | 0.157 | -0.102 | 0.023 |
| P | 0.194 | 0.998 | 0.003* | 0.153 | 0.468 | 0.308 | 0.509 | 0.882 | |
| 下口咽横截面积 | rs | 0.003 | -0.189 | 0.279 | 0.131 | -0.159 | 0.034 | -0.212 | 0.072 |
| P | 0.983 | 0.220 | 0.067 | 0.395 | 0.304 | 0.826 | 0.167 | 0.641 | |
| 咽下横截面积 | rs | -0.057 | -0.026 | 0.319 | -0.026 | -0.080 | -0.011 | -0.205 | -0.092 |
| P | 0.713 | 0.866 | 0.035* | 0.866 | 0.606 | 0.943 | 0.181 | 0.552 |
Tab.4
Changes in the upper airway at different amounts of mandibular recession"
| 测量项目 | B点后退量<4 mm(15例) | B点后退量4~7 mm(15例) | B点后退量>7 mm(14例) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 平均值 | 标准差 | 变化率 | P | 平均值 | 标准差 | 变化率 | P | 平均值 | 标准差 | 变化率 | P | ||
| 气道体积/mm3 | |||||||||||||
| 总气道 | -1 626.5 | 2 780.6 | -8.28% | 0.040* | -2 371.8 | 3 482.3 | -11.37% | 0.008* | -7 489.5 | 5 879.2 | -26.93% | 0.002* | |
| 口咽区 | -1 446.2 | 2 017.8 | -10.19% | 0.015* | -1 782.4 | 3 200.1 | -10.47% | 0.012* | -6 166.4 | 4 648.7 | -29.86% | 0.002* | |
| 上口咽区 | -1 356.0 | 1 773.7 | -16.20% | 0.010* | -467.2 | 1 709.2 | -4.73% | 0.173 | -3 150.1 | 3 285.8 | -27.37% | 0.004* | |
| 下口咽区 | -724.9 | 1 994.9 | -7.88% | 0.181 | -1 261.9 | 1 825.1 | -16.61% | 0.017* | -3 055.6 | 2 411.3 | -30.93% | 0.002* | |
| 咽下区 | -248.3 | 1 123.1 | -3.13% | 0.406 | -483.7 | 778.1 | -9.32% | 0.023* | -1301.4 | 1 662.4 | -17.97% | 0.012* | |
| 正中矢状面纵截面积/mm2 | |||||||||||||
| 总气道 | -39.5 | 90.3 | -4.58% | 0.112 | -60.8 | 100.9 | -6.53% | 0.010* | -187.3 | 152.7 | -16.55% | 0.002* | |
| 口咽区 | -33.1 | 70.9 | -5.58% | 0.092 | -39.1 | 77.0 | -5.29% | 0.011* | -147.9 | 98.6 | -17.55% | 0.001* | |
| 上口咽区 | -36.2 | 52.0 | -8.70% | 0.017* | -5.1 | 50.5 | -0.57% | 0.222 | -70.1 | 81.2 | -14.47% | 0.005* | |
| 下口咽区 | -10.7 | 63.4 | -3.49% | 0.525 | -31.4 | 51.5 | -9.50% | 0.030* | -76.9 | 61.4 | -19.03% | 0.000* | |
| 咽下区 | -9.5 | 44.1 | -1.28% | 0.416 | -17.7 | 44.9 | -4.51% | 0.114 | -24.9 | 71.0 | -3.54% | 0.001* | |
| 最小横截面积/mm2 | |||||||||||||
| 总气道 | -29.5 | 35.6 | -16.93% | 0.006* | -23.1 | 50.2 | -8.49% | 0.031* | -89.8 | 64.0 | -39.97% | 0.001* | |
| 口咽区 | -26.7 | 41.5 | -14.37% | 0.026* | -32.4 | 40.8 | -20.50% | 0.001* | -98.1 | 81.3 | -40.78% | 0.001* | |
| 上口咽区 | -22.6 | 42.8 | -10.51% | 0.060 | -27.2 | 60.6 | -13.25% | 0.028* | -89.9 | 65.4 | -36.21% | 0.002* | |
| 下口咽区 | -34.7 | 68.7 | -11.47% | 0.070 | -42.4 | 51.4 | -21.92% | 0.001* | -107.1 | 97.1 | -36.06% | 0.002* | |
| 咽下区 | 5.5 | 104.4 | 12.14% | 0.842 | -13.9 | 68.7 | 10.39% | 0.177 | -62.2 | 91.7 | -19.49% | 0.025* | |
Tab.5
Preoperative and postoperative minimal cross-sectional area risk for different mandibular recessions"
| B点后退量 | 术前最小横截面积危险度秩平均值 | 术后最小横截面积危险度秩平均值 | Z | P |
|---|---|---|---|---|
| <4 mm | 13.43 | 16.68 | -1.383 | 0.167 |
| 4~7 mm | 13.79 | 17.03 | -1.119 | 0.263 |
| >7 mm | 11.00 | 18.00 | -2.985 | 0.003* |
| [1] | Abbasi S, Rahpeyma A, Shooshtari Z, et al. Bimaxillary orthognathic surgery does not induce obstructive sleep apnea in skeletal class Ⅲ patients[J]. J Oral Maxillofac Surg, 2022, 80(8):1340-1353. |
| [2] | Parappallil CJ, Parameswaran R, Vijayalakshmi D, et al. A comparative evaluation of changes in soft tissues after single-jaw surgery and bimaxillary surgery in skeletal class Ⅲ patients[J]. J Maxillofac Oral Surg, 2018, 17(4):538-546. |
| [3] | Tan SK, Tang ATH, Leung WK, et al. Three-dimensional pharyngeal airway changes after 2-jaw orthognathic surgery with segmentation in dento-skeletal class Ⅲ patients[J]. J Craniofac Surg, 2019, 30(5):1533-1538. |
| [4] |
Park JH, Kim HS, Choi SH, et al. Changes in position of the hyoid bone and volume of the pharyngeal airway after mandibular setback: Three-dimensional analysis[J]. Br J Oral Maxillofac Surg, 2019, 57(1):29-35.
doi: S0266-4356(18)30674-0 pmid: 30598316 |
| [5] |
Bin LR, Filho LI, Yamashita AL, et al. How does bimaxillary orthognathic surgery change dimensions of maxillary sinuses and pharyngeal airway space?[J]. Angle Orthod, 2020, 90(5):715-722.
doi: 10.2319/120919-782.1 pmid: 33378484 |
| [6] | Steegman R, Hogeveen F, Schoeman A, et al. Cone beam computed tomography volumetric airway changes after orthognathic surgery: A systematic review[J]. Int J Oral Maxillofac Surg, 2023, 52(1):60-71. |
| [7] | Irani SK, Oliver DR, Movahed R, et al. Pharyngeal airway evaluation after isolated mandibular setback surgery using cone-beam computed tomography[J]. Am J Orthod Dentofacial Orthop, 2018, 153(1):46-53. |
| [8] | AlQahtani F, George JM, Bishawi K, et al. Comparison of oropharyngeal airway dimensional changes in patients with skeletal Class Ⅱ and Class Ⅲ malocclusions after orthognathic surgery and functional appliance treatment: A systematic review[J]. Saudi Dent J, 2021, 33(8):860-868. |
| [9] | Rückschloß T, Ristow O, Jung A, et al. The relationship between bimaxillary orthognathic surgery and the extent of posterior airway space in class Ⅱ and Ⅲ patients-A retrospective three-dimensional cohort analysis[J]. J Oral Maxillofac Surg Med Pathol, 2021, 33(1):30-38. |
| [10] | Ngan P, Moon W. Evolution of Class Ⅲ treatment in orthodontics[J]. Am J Orthod Dentofacial Orthop, 2015, 148(1):22-36. |
| [11] | Karaaslan S, Tüz HH, El H, et al. Three-dimensional evaluation of upper airway changes after bimaxillary surgery of skeletal class 3 patients[J]. J Craniofac Surg, 2023, 34(3):996-1000. |
| [12] | 聂萍, 陶丽, 朱妍菲, 等. 2种不同正颌术式对骨性Ⅲ类错𬌗畸形患者上气道形态的影响[J]. 上海口腔医学, 2018, 27(3):280-284. |
| [13] | Havron AG, Aronovich S, Shelgikar AV, et al. 3D Airway changes using CBCT in patients following mandibular setback surgery ± maxillary advancement[J]. Orthod Craniofac Res, 2019, 22(Suppl 1):30-35. |
| [14] | Guijarro-Martínez R, Swennen GRJ. Three-dimensional cone beam computed tomography definition of the anatomical subregions of the upper airway: A validation study[J]. Int J Oral Maxillofac Surg, 2013, 42(9):1140-1149. |
| [15] |
Ding XF, Suzuki S, Shiga M, et al. Evaluation of tongue volume and oral cavity capacity using cone-beam computed tomography[J]. Odontology, 2018, 106(3):266-273.
doi: 10.1007/s10266-017-0335-0 pmid: 29468332 |
| [16] | Brito FC, Brunetto DP, Nojima MCG. Three-dimensional study of the upper airway in different skeletal Class Ⅱ malocclusion patterns[J]. Angle Orthod, 2019, 89(1):93-101. |
| [17] | Giralt-Hernando M, Valls-Ontañón A, Haas Junior OL, et al. What are the surgical movements in orthognathic surgery that most affect the upper airways? A three-dimensional analysis[J]. J Oral MaxillofacSurg, 2021, 79(2):450-462. |
| [18] | Souza Pinto GN, Iwaki Filho L, Previdelli ITDS, et al. Three-dimensional alterations in pharyngeal airspace, soft palate, and hyoid bone of Class Ⅱ and Class Ⅲ patients submitted to bimaxillary orthognathic surgery: A retrospective study[J]. J Craniomaxillofac Surg, 2019, 47(6):883-894. |
| [19] | Resnick CM, Middleton JK, Calabrese CE, et al. Retropalatal cross-sectional area is predictive of obstructive sleep apnea in patients with syndromic craniosynostosis[J]. Cleft Palate Craniofac J, 2020, 57(5):560-565. |
| [20] |
Deyoung PN, Bakker JP, Sands SA, et al. Acoustic pharyngometry measurement of minimal cross-sectional airway area is a significant independent predictor of moderate-to-severe obstructive sleep apnea[J]. J Clin Sleep Med, 2013, 9(11):1161-1164.
doi: 10.5664/jcsm.3158 pmid: 24235897 |
| [21] |
Marcussen L, Stokbro K, Aagaard E, et al. Changes in upper airway volume following orthognathic surgery[J]. J Craniofac Surg, 2017, 28(1):66-70.
doi: 10.1097/SCS.0000000000003206 pmid: 27893557 |
| [22] | Zhao YL, Li XY, Ma JG. Combined application of pharyngeal volume and minimal cross-sectional area may be helpful in screening persons suspected of obstructive sleep apnea (OSA)[J]. Sleep Breath, 2022, 26(1):243-250. |
| [23] |
Zhang ZQ, Wang SZ, Li J, et al. Quantification of pharyngeal airway space changes after two-jaw orthognathic surgery in skeletal Class Ⅲ patients[J]. BMC Oral Health, 2023, 23(1):345.
doi: 10.1186/s12903-023-03075-y pmid: 37264397 |
| [24] | 龚依玲, 樊蓉, 常新. 骨性Ⅲ类患者正颌手术后上气道变化预测方法的研究现状[J]. 口腔医学, 2023, 43(10):955-960. |
| [25] | Ghosh A, Ray A. “Converting a bi-jaw surgery to a single-jaw surgery:” Posterior maxillary dentoalveolar intrusion with microimplants to avoid the need of a maxillary surgery in the surgical management of skeletal Class Ⅲ vertical malocclusion[J]. APOS Trends Orthod, 2016, 6: 218-227. |
| [26] | 罗世逸, 羊书勇, 吴坡, 等. 双颌前徙术配合颏成形术对OSAHS患者气道容积的影响[J]. 西南国防医药, 2020, 30(1):38-40. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||